Keywords: alopecia, female alopecia, menopause, postmenopause, estrogen, phytoestrogen, menopausal hair loss, clinical trial, agnocaste, biotin
STUDY OF A NUTRACEUTICAL AND A PHYTOTHERAPEUTIC LOTION IN WOMEN WITH POST-MENOPAUSAL FEMALE ALOPECIA
STUDY OF A NUTRACEUTICAL AND A PHYTOTHERAPIC LOTION IN POST-MENOPAUSAL WOMEN AFFECTED BY FEMALE ALOPECIA
Lucia Villa, Giovanni Profeta, Francesca D'Anna, Massimiliano Cametti, Bartalini Luisa, Cuffaro Lorena and Andrea Marliani
Introduction: postmenopausal female alopecia
In female patients, estrogen deficiencies in the hair follicle can lead to the manifestation ofLudwig-type Female Androgenetic Alopecia. In fact, as is well known, the hair cycle is controlled by sex hormones, both estrogen and androgen, present and produced at the follicular level. A fledgling branch of medical science is in fact “intracrinology” which is concerned with studying the intracellular “intracrine” interactions of hormones and how they profoundly affect various biological processes. Specifically at the intrafollicular level, two sex hormones play a very important role in the physiological regulation of the hair cycle: Dihydrotestosterone andEstrone.
Estrone maintains the mitotic activity of the hair matrix, lengthens the duration of the anagen phase, and activates hair stem cells; DHT, on the other hand, exerts an opposite action, terminating the anagen phase by bringing the hair into telogen and the follicle into catagen.
Why counteract DHT to promote regrowth?
The presence of DHT, produced at the hair level by 5-alpha-reductase type I is the main cause of male Androgenetic Alopecia. However, in women, the blood presence of testosterone, and consequently of DHT at the follicular level is normally very low, except in very rare cases of abnormal hormone production, often due to tumors. It is possible to assume that, excluding other causes of an autoimmune nature or from nutritional deficiencies, female androgenetic ALOPECIA is caused by a deficiency of estrone at the level of the hair follicle.
Intake of phytoestrogens may help to make up for this deficiency at the peripheral level. However, it is interesting how phytoestrogens have a peculiar biochemical behavior within the human body. In fact, from medical meta-analysis studies conducted on Asian populations in which the diet is high in phytoestrogen-rich vegetables, particular cytoprotective characteristics of phytoestrogen have been found to protect the breasts, female genitalia, and uterine mucosa from the onset of cancer. It is likely that this is due to the greater affinity of phytoestrogen for estrogen-binding cell receptors than for endogenous female hormones, thus preventing their binding, and preventing the aggravation of estrogen-sensitive tumor situations with an anti-estrogenic action. In contrast, at the skin and hair level, phytoestrogens have a true estrogenic action. The biochemical reason behind this peculiarity of action remains unclear.
Estrone maintains the mitotic activity of the hair matrix, lengthens the duration of the anagen phase, and activates hair stem cells; DHT, on the other hand, exerts an opposite action, terminating the anagen phase by bringing the hair into telogen and the follicle into catagen.
However, as a result of what has just been discussed, it is apparent that, improving estrogen concentration at the level of the hair bulb is a viable therapeutic approach for Alopecia Femminile estrone deficiency.
Objective of the study
The objective of the study is to evaluate the efficacy and tolerability of a treatment consisting of a nutraceutical (Restax Donna Plus 30cps) and a topical lotion (Restax Donna Lotion 100ml) containing phytotherapeutic active ingredients in postmenopausal female patients and has as its primary end-point, the evaluation of hair status before and after treatment. This assessment will be carried out by means of an evaluation form, completed by the physician at the beginning of treatment and after 8 months, on which the intensity of clinical symptoms associated with Alopecia is noted.
Materials and methods: how to treat postmenopausal female alopecia?
A total of 106 postmenopausal patients participated in the study; each patient was asked to take 1 capsule of Restax Donna Plus supplement daily, during dinner, and to apply Restax Women’s Lot ion every other day a minimum of 3 times per week, applying 15 sprays to the affected areas, to damp or dry hair that was not necessarily washed before each application.
The researcher after examination and history of the patient then completed the questionnaire at T0 and T8, assessing clinical symptoms such as pull test result, presence of trichodynia and itching, using a scale of 0 to 5, where 5 indicated a very strong presence of the symptom in question, 0 indicated its absence. The researcher also rated the average hair diameter, with a value of 5 for an observed value of very good hair diameter and 0 for an observed value indicating extremely thin hair. The physician then commented on the clinical situation of the patient in question, with a value of 0 indicating a negative clinical situation and a value of 5 indicating a very positive clinical situation. As additional clinical data, the level of postmenopausal Female Alopecia was noted according to Ludwig’s scale, using numbers from 0 to 7, with 0 indicating total absence of hair in the apical area of the head and 7 indicating perfectly normal hair. In addition, satisfaction values for efficacy and tolerability were expressed by the physician and patient at the end of the study.
Features of RestaX Women's Plus and RestaX Women's Lotion.
Nutraceutical Restax Woman Plus 30 cps:
Chasteberry dry extract, 200 mg, 0.5% agnuside: A natural progestin that acts on adenylyl cyclase activity, it reduces the duration of catagen and telogen phases as it hampers the 5-alpha-reductase metabolic pathway by reducing follicular DHT synthesis; it also helps activate aromatase, which converts excess testosterone to estrone.
Hops dry extract, 200mg, 0.4% rutin: Containing phytoestrogens that activate the anagen phase of the hair, among the phytoestrogens present in Hops, of particular importance ishopein, the most potent phytoestrogen known to date. This molecule is characterized by estrogenic activity equal to that of significantly higher concentrations of genistein or daidzein, as much as 50-100 times higher, this due to the greater bioavailability of hopein compared to other phytoestrogens. It performs an action of physiological promotion of the anagen phase.
Kudzu dry extract, 150 mg, 40% in isoflavones: Kudzu is a plant native to East Asia, rich in isoflavones such as genistein, daidzein and puerarin. It is used as a source of phytoestrogens, due to which it reduces hot flashes, stimulates bone remineralization, calms nervous hunger, and aids proper cardiovascular function. Kudzu extract, among other things also has an adaptogenic function, stimulating the production of serotonin and dopamine and balancing mood and the sleep-wake cycle, which is particularly useful in female patients prone to Alopecia, since for them hair loss is also associated with a strong negative psychological impact.
Resveratrol from Polygonum cuspidatum root , 50 mg: Powerful antioxidant, and anti-inflammatory, slows cellular aging by protecting biological molecules from oxidizing agents.
Niacin 25 mg: Also known as Vitamin B3 or PP, it is involved in the production of NADH, a coenzyme of fundamental importance in all cellular metabolic processes; its deficiency leads to progressive hair loss and weakening.
Biotin 450 ug: Also known as vitamin B8 or Vitamin H, it is an essential nutrient because the human body is incapable of synthesizing it on its own. It aids the absorption of nutrients at the cellular level and performs an important function in fat and carbohydrate metabolism. Its deficiency leads to thinning and loss of color in hair.
Piper nigrum root dry extract, 7 mg, 95% in piperine: Possible anti-androgen as it has demonstrated 5-alpha-reductase inhibitory activity in vitro, black pepper extract enhances the absorption of other active ingredients, increasing their BIOAVAILABILITY.

Whereas as for Restax Women’s Lotion 100mL :
Main solvent: 80% v/v water ethyl alcohol mixture, to best solubilize all product components
Dimethyl Sulfone 0.5%
It enhances the solubilization and release of all active ingredients, promoting their passage through the superficial keratin layer of the dermis.
Sphinganine 0.3%
It is a natural skin sphingolipid of fundamental importance for its biological functions. It acts physiologically on hair loss by rebalancing the hair cycle, nourishing the hair follicle and improving scalp health.Sphinganine balances the natural hair cycle and promotes the Anagen phase by slowing down the telogen phase through physiological 5-alpha reductase inhibition action.
Chasteberry 0.7%
Agnuside, contained in Agnocaste extract, is a natural progestin that acts by going to stimulate the skin-level activity of P450 aromatase, and also has a moderate anti-androgenic action by inhibiting DHT synthesis.
This stimulates adenylate cyclase activity by lengthening the ANAGEN phase. Agnocaste also regulates progesterone levels, influencing the Progesterone/Estrone ratio in favor of the former.
Hops 0.35%
Hops extract contains phytoestrogens which go on to physiologically increase follicular estrone levels, contributing to the activation and elongation of the ANAGEN phase. Specifically, Hops contains Hopein, the most potent phytoestrogen currently known, which exhibits abilities to bind to estrogen receptors comparable to those of significantly higher concentrations (50-100 times) of soy phytoestrogens; this is due to the higher bioavailability of hopein compared to these substances.
Ribes nigrum 0.7%
Currant extract is a natural anti-inflammatory and has the ability to block the synthesis of anti-inflammatory cytokines locally, which are often involved in the ultimate loss of the hair follicle.
Results of the study on postmenopausal female alopecia
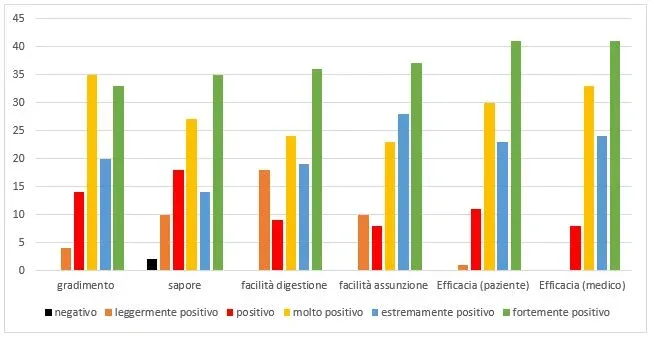
A total of 106 postmenopausal patients, ranging in age from 44 to 95 years, participated in the study; the average age of the patients was 61.77 years. Following the 8 months of therapy, patients were asked about their degree of satisfaction with the therapy by asking questions regarding the taste of the product, its efficacy (rated by both the doctor and the patient), ease of digestion, and ease of intake. The evaluation was possible through a form with values from 0 to 5, where 0 indicated a negative liking value and 5 a strongly positive value. No patients reported negative judgments regarding the therapy they underwent, except for two patients who judged the taste of the nutraceutical taken as not pleasant. The ratings for the other categories were mainly on the value of very positive (3) or strongly positive (5).
As for clinical data, on the other hand, the rating was expressed in values from 0 to 7 for Ludwig’s scale and again from 0 to 5 for each other category. The initial value of alopecia level according to the Ludwig scale stood at a value of 3.49, indicating a situation of already visible apical thinning and a medium alopecia, while at the end of the study the value went to a value of 5.06 indicating a condition of very moderate alopecia with slight thinning, demonstrating an improvement of 30.97% over the initial value. For clinical assessment, pull test, trichodynia and itching lower values indicated less presence of the problem or better clinical assessment, for hair diameter on the other hand, higher values identified larger diameters. Specifically, at the beginning of the study, out of 107 patients, 82.08% reported positive pull test results, 53.77% reported suffering from trichodynia and 42.28% reported scalp itching. At the end of the study, the same symptoms were reported by a very small number of patients, specifically positive pull test was in 35.85% of patients, trichodynia in 12.26 and scalp itching in 5.66, with a substantial reduction in the number of patients suffering from these symptoms. In addition, the average intensity of these symptoms has also been decreasing, in fact The initial values stood at 1.81; 1.27 1.08 for pull test, trichodynia and itching respectively, indicating a sitation of positive pull test, trichodynia and mild itching.

At the end of the study these values were reduced to 0.53; 0.16 and 0.08 with an average decrease in symptoms of 70.83% for pull test, 87.40% for trichodynia and 92.98% for itching. Average hair diameter also went up, with a reported initial mean value of 2.63 out of 5 and a final value of 3.91 out of 5, a 48.42% improvement. In addition to this, out of 106 women participants, 2 reported reporting side effects, but these were minor and did not prevent discontinuation of the treatment. Specifically, one patient, 82 years old, reported developing hemorrhoids as a side effect as a result of taking the product, however, the problem was not particularly severe and resolved quickly by taking an antihemorrhoid medication. A second patient, age 51 complained of constipation problems that arose a few weeks after starting treatment: again, the problem resolved quickly and without particular discomfort for the patient.
Conclusions of the study
The study indicates a positive correlation between treatment with taking the nutraceutical “Restax Woman Plus” and the application of the lotion “Restax Woman Lotion“, and the decrease of female Alopecia symptoms. Moreover, the products in question proved to be substantially safe and with high tolerability: any side effects, where present, were limited in time and did not affect the ability to complete the therapy or significantly diminish the quality of life of the patients who suffered from them. Given these results, it is reasonable to conclude that a combination of the nutraceutical and the lotion under study can be used as a viable answer to the problem of Female Alopecia in old age.
Bibliographical references
Arnoux M.: “Administration percutanéedesstroïdes” NouvPresMéd 1979; 8: 3797;
Cherif-Cheik J.L., De Lignieres B.: “Traitement de la séborrhéeducuirchevelu par la progesterone percutanée.” Thérapeutique Sem. deshopitaux de Paris 1974; 50: 489.
Fayolle J.: “La progesteronepercutanéedans le traitement de l’acne et desétatsséborrheiques de la peau et ducuirchevelu. Etude de 66 cas” Lyon Medical 1975; 233: 1303.
Feldmann R.J., Maibach H.I.: “percutaneous penetration of steroids in man” J Invest Dermatol 1969; 52: 89.
Grant, P., & Ramasamy, S. (2012). An update on plant derived anti-androgens. International journal of endocrinology and metabolism, 10(2), 497.
Hirata N1, TokunAlopecia M, Naruto S, Iinuma M, Matsuda H “Testosterone 5alpha-reductase inhibitory active constituents of Piper nigrumleaf.” Biol Pharm Bull. 2007 Dec;30(12):2402-5.
Kim, J. E., Jeong, H., Hur, S., Lee, J., & Kwon, O. (2020). Efficacy and Safety of Kudzu Flower-Mandarin Peel on Hot Flashes and Bone Markers in Women during the Menopausal Transition: A Randomized Controlled Trial. Nutrients, 12(11), 3237.
Manfredi G.: “Considerations on the antiandrogenic activity of progesterone,” Med Est 1981; 4: 160.
Marliani A.: “The medical therapy of common baldness,” Etruria Medica, Florence, 1992.
Mauvais-Jarvis P., Kuttenn F., Baudod N.: “Inhibition of testosterone conversion to dihydrotestosterone in man treated percutaneously by progesterone” J Clin Endocrinol Metabol 1974; 38: 142.
Prince V.H.: “Testosterone metabolism in the skin,” Arch. Derm 1975; 11: 1496.
Reuter, J., Merfort, I., & Schempp, C. M. (2010). Botanicals in dermatology. American journal of clinical dermatology, 11(4), 247-267.
Wang, M., Wu, Q. L., Simon, J. E., Jin, Y., & Ho, C. T. (2005). Chemistry, pharmacology, and quality control of selected popular Asian herbs in the US market (pp. 73-102). Marcel Dekker, Inc., New York.
Zappalà F., Caruso A., Giardina A., Randazzo S.D.: “Therapeutic activity of progesterone 0.5% solution in some androgen-dependent dermatoses” Med Est 1983; 3: 113.